



My midlife physical results (2023)
Every year I have a physical. Here are the highlights of my latest one.


Because I got such positive feedback on my supplement post, I wanted to share more about my personal journey.
It’s important to remember that biomarkers are individual and can be affected by many different things including genes and underlying factors. And numbers don’t tell the whole story of health.
Also, my intent is always to provide education so you can get more out of your relationship with healthcare providers. It’s not to replace medical advice.
But I do believe biomarkers are important and a place we can see progress and get answers. But before getting into the details, let me update you on where I am in the menopause transition.
Hello late perimenopause
I’m 54 and in late perimenopause. This post defines all the stages. Late perimenopause is defined as more than 60 days without a period. Last year after my last physical in September, I finally passed the-60-day mark. It was 90 days to be exact.
During this time off, I had vaginal dryness and irritation and asked my doctor for vaginal estrogen, which has been a lifesaver. I had a couple of light periods after the three-month hiatus and then had another three-month break following two more light periods.
I thought light periods were becoming a norm, but out of nowhere, I experienced one of my old, heavier periods. This proves you can never be too sure.
As for symptoms, I’m still feeling good. No sleep issues and I don’t have hot flashes or high anxiety.
At this rate, the earliest I will be menopausal is 55. Menopause is defined as an entire year without a period and April is my birthday. Bleeding is a good indicator of estrogen status as it builds up the uterine lining. Overall, my estrogen has been declining. Studies show estrogen declines about two years before the final period. So, it’s coming.
Pre-work for my physical
About a month before my physical, I start taking my blood pressure at home. I don’t look at the number and my monitor stores the readings for me. To see why I do this, check out my post about my white coat hypertension turned bp phobia.
I check it about 2-3 times per week and try to get as many readings as I can. I take it around 9 am and let myself have a little coffee but not much (about ½ cup). I also allow time to get my labs done and usually ask my doctor to add in a few things.
This time I wanted to add a full iron panel and Free T4. I like getting an early appt so I’m fasting around 13 hours, the same every time. If you have regular cycles, you’ll want to schedule blood work to be around the same time because labs can vary based on where you are on your cycle.
A day or two before my physical, I look at my blood pressure numbers, which still gets me riled up. They were good – phew! They ranged from 106/66-121/60. I email them to my doctor.
I also check my apple watch for my resting heart rate. It ranges from 58-60, but sometimes down to 55 and up to 62. Resting heart rate is supposed to be taken right before you get up in the morning, but if I do that, my heart rate spikes.
Getting my biomarkers
I get the labs before my doctor visit. This is when I review them, write down any questions, and do research if I need to. Now that I’m further along with perimenopause, I braced myself for changes. But my doctor says that usually happens more post menopause.
I finally put all my labs in one chart from 1999 onward. Let’s start with red blood cell markers.
This is my sad story of my iron deficient days. As you can see, I never had a ferritin run until I was anemic, which just boggles my mind. Ferritin is the most accurate measure of iron status. The clue that my iron was running low occurred in 2014 when my red blood cell distribution width (RDW) was high.
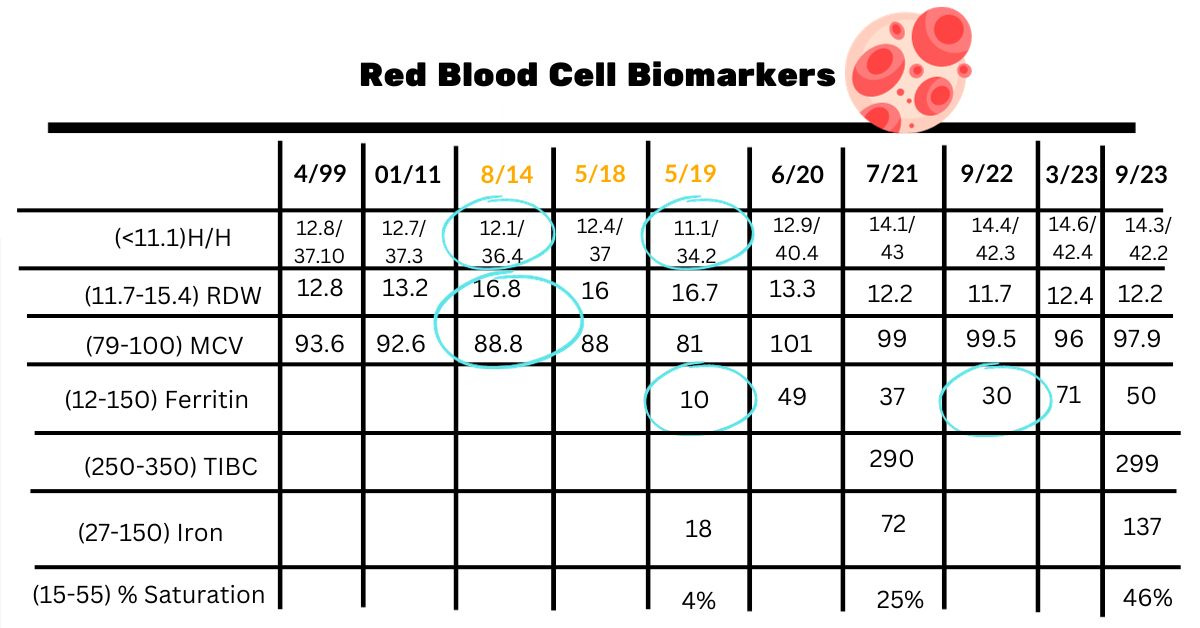
RDW is the variation in the size of red blood cells. This means that when it’s high, there’s more variation in red blood cell size instead of being more uniform. Also, my hemoglobin and hematocrit started to decline even though I wasn’t officially anemic. I went four years until I had another physical and my labs were pretty the same. Those were four tired years!
If you have ample periods, month after month, this could be you!
Another clue was my mean corpuscular volume (MCV). This is the size of your red blood cells. When this declines, it usually means iron is an issue. And when it is high, B12 and folate should be looked at. I have discovered when I’m iron replete; I have a normal/high MCV. A couple years back I got a peripheral blood smear, and folate and all was normal.
But back to where I am now. Last September I experienced vague but familiar iron deficient symptoms and sure enough my ferritin had gone back down to 30. After that I went three months without a period and was still taking iron. When I had it checked a few months later, my ferritin was up to 70. That’s when I stopped the iron maintenance dose of 1-2 times per week.
I’m good now with a ferritin of 50 and likely will only take iron if I continue to have more heavy periods. What’s interesting is hemoglobin and hematocrit have increased. When you first take iron, it’s supposed to “fill up” hemoglobin and hematocrit first before ferritin. But two years later, mine went up more significantly.
I do notice that my heart rate is more stable during exercise. It used to get up there! It must be that I have a better capacity for oxygen delivery.
This time around, I wanted to check to see that I had available iron, so got the full panel. My iron saturation was a bit high, but my doctor says this is highly variable. It’s important to note that when ferritin and iron saturation are high, you want to ask your healthcare provider about hemochromatosis. This can reveal itself in some women when periods stop either due to menopause or birth control.
Cardiovascular biomarkers
It’s interesting that my highest LDL cholesterol was in 2001. That is when I moved to New York and ate out a lot (lol). For most of my 40s, it hovered around 80 and then started inching up. I was happy it stayed close to 90. Cholesterol goes up about 10% with menopause.
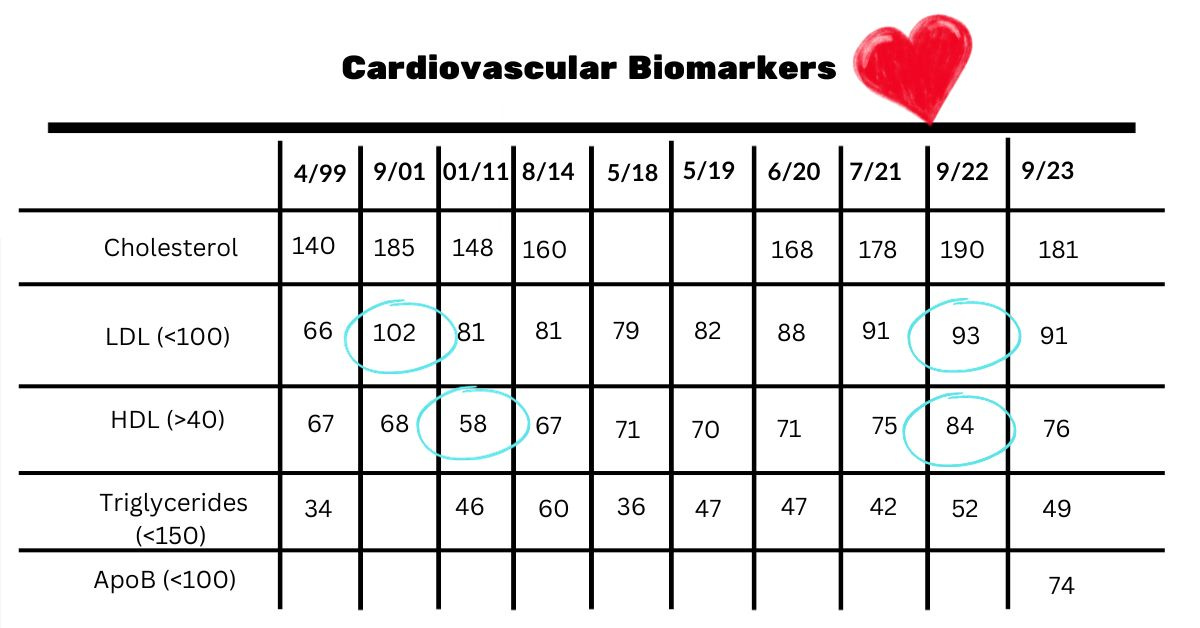
What has been most surprising is how my HDL has increased. It dipped in 2011 and I think it’s because I was having an ulcerative colitis flare. Last year, my HDL was 84, and it surprised me. I think getting my omega-3 index up is behind this. And overall, I eat more fish and nuts than I used to. Omega-3, heathy fats, and exercise all can increase HDL.
Most of you probably know HDL is the good cholesterol and LDL is not-so-good. But recent research shows HDL isn’t as straightforward as researchers thought. The thinking now is that as we get older, it’s more of a neutral marker. So, it may not make up for a high LDL. But HDL does play a role in insulin resistance, as I discuss in the next section.
If you’re familiar with Peter Attia’s work, he’s a big fan of ApoB as a key cardiovascular marker. This is supposed to be superior to cholesterol. It’s hard to find what is ideal, and I think they’re still figuring it out. But at least under 90. I got mine checked through walk in lab and it was 74.
I wonder if my good marks may also be because of my latest kick in estrogen. In a 2010 study, HDL increased, and LDL cholesterol/triglycerides declined as estrogen levels rose during the menstrual cycle (read about it here). They reach their lowest in the luteal phase, right before a woman’s period.
This is why always taking it at the same time in your cycle is helpful. If you’re in perimenopause, this is near impossible.
I’m a big fan of the portfolio diet–cholesterol-lowering foods — which I talk about in this post.
If your cardiovascular markers suddenly get out of whack, be sure to check in with your thyroid markers, which is what we’re highlighting next.
Thyroid biomarkers
A 2022 study looked at 10,747 adults that were separated into hypothyroidism (311), subclinical hypothyroidism (5015), hyperthyroidism (203) and subclinical hyperthyroidism (118). Dyslipidemia (high triglycerides, low HDL, high LDL) was closely linked to thyroid dysfunction, which the study found was also related to menopause.
Subclinical hypothyroidism poses a stronger risk probably because it usually goes untreated. Monitoring thyroid biomarkers is important, especially when your cardiovascular labs get out of whack.
Overall, mine have been good. I had my highest TSH on 6/20. That was when I added a multi with iodine and drops on alternate days (Just the RDA, not high levels which are not recommended). But many micronutrients play a role in thyroid health, including vitamin D, iron, magnesium, selenium, and zinc.
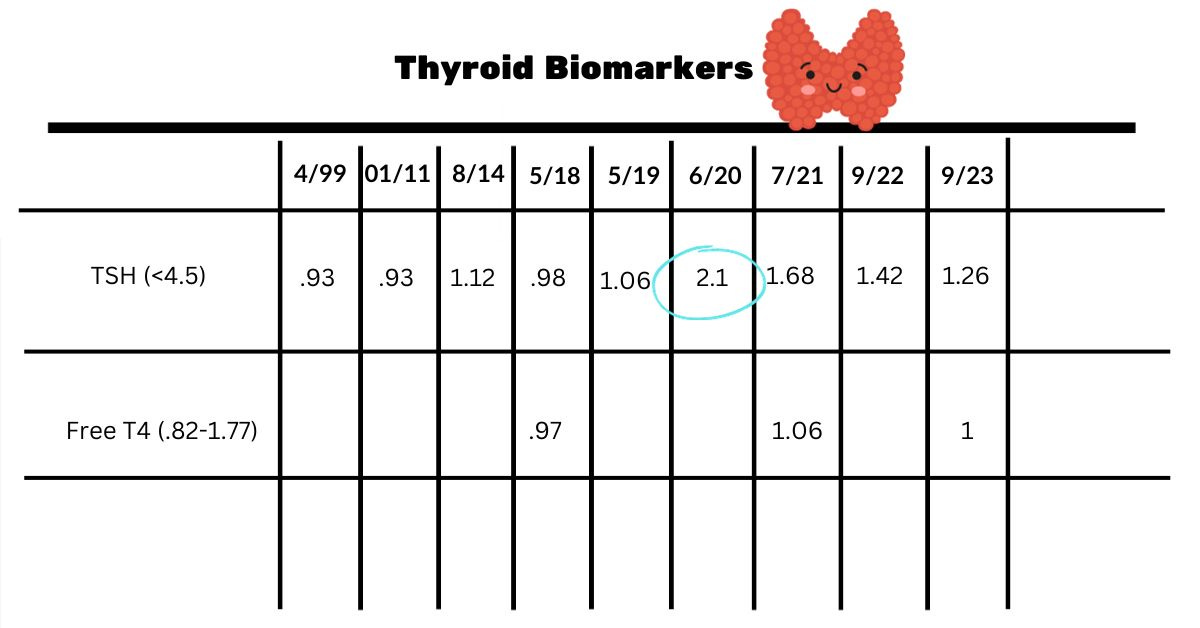
Conventional doctors rarely consider nutrition when thyroid markers change, and we don’t have a lot of research. But it’s important during this time to ensure you are at least getting the recommended amounts along with checking nutrition biomarkers.
If you notice a rise in TSH, you can ask for an anti-TPO to check for an autoimmune issue.
Blood sugar/insulin
You hear a lot about insulin resistance at midlife. It is a risk. In my biomarker guide, I include tests for insulin. So far, I’ve had only the basic ones done. But there is a calculation you can do to see if you are at risk.
Divide triglycerides by HDL as shown in the chart. According to a 2021 study, >1.65 in women has 80% sensitivity in identifying insulin resistance. You can ask for a fasting insulin if you feel you are at risk.
You can see on 5/18 my hemoglobin A1C shot up to 5.5. Hemoglobin A1C is the average of blood sugars over three months. I remember thinking that I was close to prediabetic, which is 5.7. Later I learned A1C can increase when you are low in iron. And that was a year before my anemia diagnosis. It went right back down and recently has been 4.9.
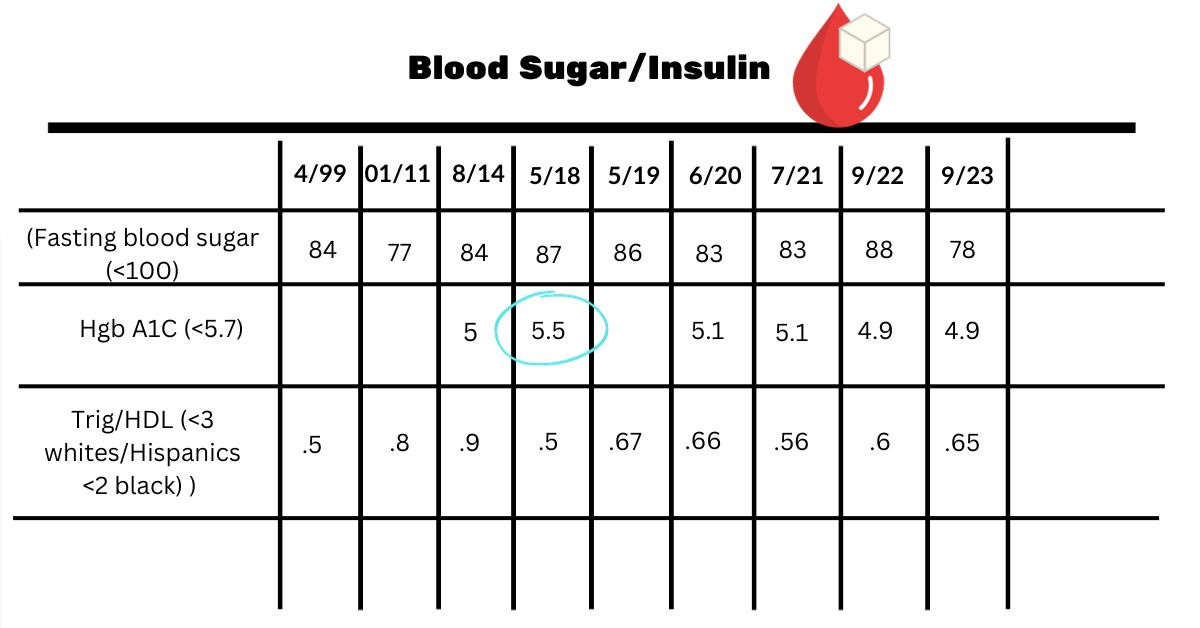
Changes I've made that could have affected my blood sugars were getting more protein at breakfast and taking those walk breaks as I talk about here.
Nutrition Biomarkers
I touched on vitamin D in my supplement post. Now, looking at all of them, I can see that by springtime, my levels used to be down closer to 30ng/ml. I’ve learned I need to take an extra 1000 IU in the winter, and I can meet my goal of 50ng/ml.
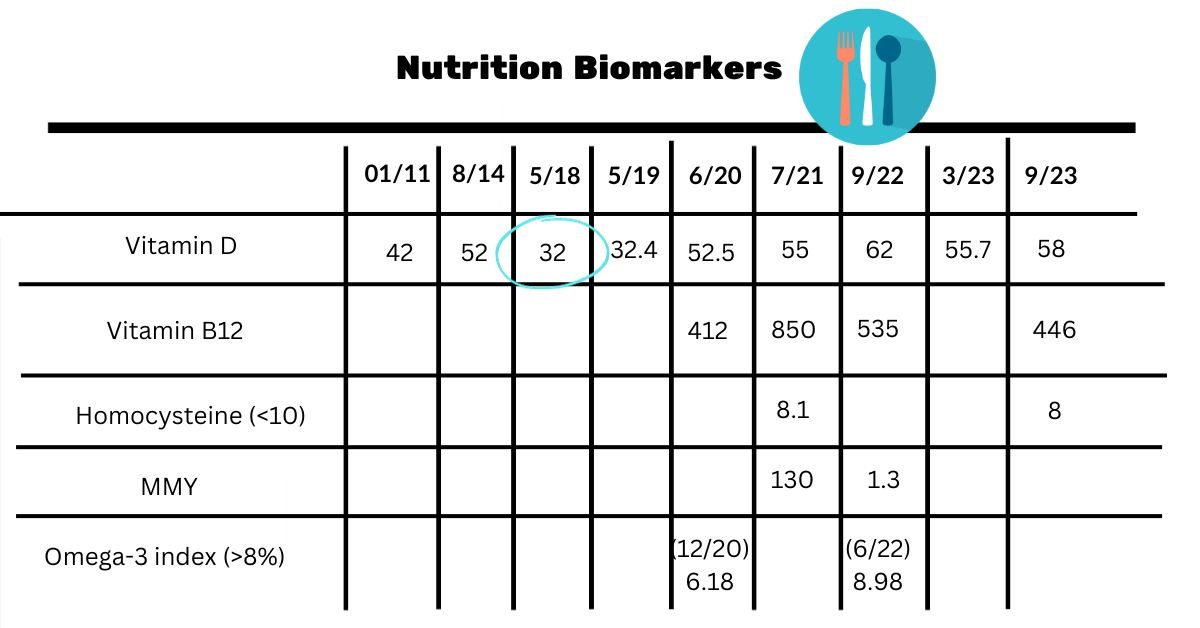
I remember getting a bad case of pneumonia in 2014. I wonder if it was the dwindling vitamin D along with low iron, both affect the immune system. This is important as flu and covid season is upon us!
After I first got my B12 checked, I started taking vitamin B12 and my numbers went up. Now I check methylmalonic acid (MMA) and homocysteine and just try to keep B12 above 500. It’s not clear if really high levels are beneficial. I’d rather get my biomarkers checked and increase as needed. I’m going to be adding B12 once or twice a week in addition to my multivitamin.
I checked homocysteine at Walk in Lab and MMA at OmegaQaunt.
Other stuff
During my physical we reviewed my labs, and the doctor did a checkup, which included a skin check. I have two slightly raised areas on my nose that could be actinic keratosis, precancerous lesions which are common. She removed them and said if I can still feel them in a month to get a referral to a dermatologist.
I got a flu shot and will also get a shingles shot at the local drugstore. Plus, I set a mammogram for January.
I know I should get an appointment with a gynecologist to look at my options as I approach menopause. The last time I had an appointment, she discovered a polyp that I had removed. To get in with this same NAMs certified doctor would take months. Ugh.
Well, that’s it for now. Have you had a physical lately? Where are you on the perimenopause journey? Would love to hear from you!