

Perimenopause is not puberty in reverse (and here's why)
Let’s stop ignoring the biggest difference between puberty and perimenopause [Aging]


People often describe perimenopause and menopause as puberty in reverse. And I disagree.
A key difference between puberty (hormone increase) and perimenopause (hormone decline) is during puberty, bodies are young. They are also anabolic bodies; meaning they are on a growth trajectory.
But at midlife we are no longer anabolic. We are at what I call the maintenance phase. This means that if we don’t do the maintenance, like with our car or home, things begin to decline. Yes, there is inevitable decline, but most of that comes after 60, towards the end of midlife.
But the biggest factor no one talks about is that we don't make adolescence only about puberty. The development stage of adolescence is from 10 to 20 (ish) and puberty is a part of that. Yet for midlife, we haven’t done that.
Instead, we’ve made midlife (for women) mostly about menopause. Because October is Menopause Awareness Month I want to talk about an ignored part of menopause. This is what precedes and continues right along with it.
Aging.
The effects of aging at midlife
I got to the point in my book writing where I kept saying “due to both aging and hormonal changes.” So, I came up with the term “aging pause.” As I see it, midlife is where aging meets menopause.
Aging is about time. And with more time on this earth, things get interesting.
Although no official definition exists, most studies I’ve read consider midlife from about age 40 to 65. The average age of menopause is right around the age of 50. This means that most women are almost halfway through midlife when menopause occurs. Estrogen begins its descent about 2 years before the last period, although for progesterone it’s more like 5 years.
We move out of the anabolic stage of growth right around the age of 30. The brain stops developing at 25, bone stops growing by 30, and muscle protein synthesis switches from growth hormone driven to a leucine trigger (meaning we need adequate protein) around 30.
This is likely why relative muscle mass and power start to decline by the third decade. And according to a 2019 study in the Journal of Osteopathic Medicine, 26% of premenopausal women (35-50) already have osteopenia, weakening of the bones. Mind you, this is before the rapid bone loss occurs during and after menopause.
Nearly 10 years after the brain is done developing and 10 years before perimenopause, around 35, we begin to lose 0.2% brain volume per year. Nitric oxide, a vital signaling molecule that keeps arteries flexible–and plaque from forming on the arterial wall–is roughly half of what it was in our 40s compared to our early 20s.
The Dunedin Study measured biological aging in a group of 1,037 mixed gender New Zealanders from birth to age 45. At each visit–ages 26, 32, 38 and 45 — they collected 19 biomarkers assessing the function and health of their bodies, quantifying it in what they refer to as the "Pace of aging.”.
Those with a faster pace of aging showed worse signs of cognitive difficulties, white matter volume loss and more difficulty with sensory motor function capacity. The researchers define biological aging as “decline that (a) simultaneously involves multiple organ systems and (b) is gradual and progressive.”
This data reveals that by the beginning of midlife, the effects of aging are a thing, even for premenopausal women. Yet there’s still plenty of time to slow it down and meet the new needs of our aging bodies. This paper perfectly states the concept of the "midlife window of opportunity."
"To achieve maximal prevention of age-related diseases, interventions to slow biological aging will need to target individuals by midlife before decades of subclinical organ decline have accumulated."
Then comes perimenopause
When a woman enters perimenopause, it shakes everything up. It’s like shining a bright spotlight on the areas that need work, both emotionally and physically.
That’s because our hormones do a lot of heavy lifting. And once they begin to change, we finally take notice, unlike the gradual aging changes.
For me, it came in the form of crippling anxiety at age 48. When I looked it up, I found many women experience anxiety at midlife. I assumed this was hormonal in nature, which is a common mistake.
Luckily, I had a history of anxiety and knew what to do. I got therapy for CBT and found the DARE program (exposure therapy) which helped immensely with my driving anxiety. Yet I still felt run down and had a high heart rate during exercise and I had those damn palpitations.
Two years later, I got diagnosed with iron deficiency anemia and did more research. I knew that I had been iron deficient without anemia for most of my 40s. Correcting this made the palpitations and heart rate issues go away for good.
What if I didn’t get help?
Let’s consider what would have happened had I not found out I was anemic. I would’ve stayed iron deficiency without anemia. Because iron and red blood cell health play important roles in the production of thyroid hormone, my thyroid could begin to experience problems.
This link between iron deficiency and thyroid dysfunction is established in pregnancy, but not in the general population. So, researchers set out to do a comprehensive study in a Spanish and thyroid disease-free population (18-93 years old). They examined the relationship between ferritin levels and markers for thyroid function–TSH, FT4 and FT3.
You can see that 60% of premenopausal women were iron deficient with a ferritin <30ng/ml which extends to about 50 when menopause occurs and goes down. But it’s still around 20% and increases slightly with age.
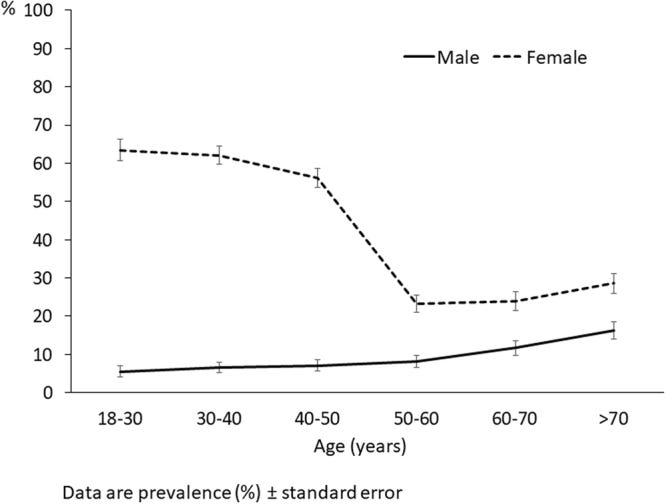
People with ferritin levels <30ng/ml had lower levels of both FT4 and FT3, showing thyroid function becomes compromised with lower iron stores.
Eventually, this could affect my cardiovascular system as subclinical hypothyroidism is known to do. I’d be more likely to have high blood pressure, cholesterol, and triglycerides.
And they would assume it was because I was menopausal, and the underlying issues would stay secret.
Why aging pause matters
We need to reach women well before menopause. But we can’t make it just about eating healthy, exercise, and weight. The only preventative measure put forth to date has been to council midlife women about weight. Can you believe that?
Midlife women need to understand how their micronutrient needs change with aging pause. Let’s please universally check ferritin, vitamin D, and vitamin B12.
Midlife women, know your biomarkers and what questions to ask and tests to get.
Let’s do bone density screenings early in midlife so women can take action sooner (instead of age 65!). Strength training will help attenuate losses in muscle and bone and has been shown to be as effective as hormone therapy in preventing bone loss.
Consider screening for adverse childhood experiences and referring women for trauma-informed therapy, as it has been shown to significantly impact health and vasomotor symptoms.
We need a screening tool for endothelial dysfunction, which is the silent precursor to heart disease (I have ideas, if any researchers are reading this). A compromised endothelium is likely a key contributor to hot flash severity, which, according to new research presented at the Menopause Society, heavily affects heart disease and dementia.
In short, we need to bring the effects of aging into the equation of menopause. Women have lived in their body for four to five decades and lots of sh%t can take place by the time changing hormones shake things up,
It’s time to build that foundation of development around menopause–defining the new needs of midlife women -- the same way we did for adolescence and puberty. If we do that, then maybe we can call perimenopause puberty in reverse.
Then we can change the name from menopause to aging pause. What do you think?
This seems so incredibly important and yet I have yet to see a doc (well there was one nurse practitioner who was amazing) who gives a flip. Of course, we also do cervical procedures with no painkiller and brush off PMDD and all manner of repro issues. Why? Misogyny?