



The gaping hole in women's health research
It's time to stop ignoring midlife women's health issues


Just last week I wrote about how the Midlife Women’s Health journal is closing its publication. The reason given was that other journals are increasing their research on midlife topics. And then I run across a study that shows, well, this isn’t happening.
A 2022 study in Journal of Women’s Health reviewed research from 2010 to 2020 in six women’s health journals (WHJ) and five general medical journals (GMJ). The analysis revealed studies focus mostly on reproductive health, including pregnancy. And this hasn’t changed since 2000!
We are woefully behind in women’s midlife health research. Let’s take a look.
Imbalance of studies
The researchers found 1483 eligible articles and compared the study topics to leading causes of diseases in women according to the Global Burden of Disease (GBD) study.
Reproductive health accounted for 44% of WHJs' topics. GMJs were close with 40%. Of the non-communicable diseases studied, cancer was way ahead at 40.5% followed by mental illness/substance abuse (22.2%), cardiovascular disease (15.5%), musculoskeletal disorders (5.7%) urology (4.4%), and digestive and nutrition (3.7%).
That last one hurt.
The top three leading causes of death in women in 2019 were cardiovascular disease, neoplasms (cancer), and chronic respiratory disease.
Although cardiovascular disease is responsible for 13.4% of disability adjusted life years (DALYs), it consisted of only 5.3% of the topics in WHJ and 3.4% in GMJ. On the other hand, reproductive conditions make up only 1.2% of DALYs, but accounted for 17.4% of topics in WHJ and 28.5% in GMJ.
Not only that, but one of the top causes of death in women, respiratory disease, accounted for only .7% in WHJ and 2.2% in GMJ.
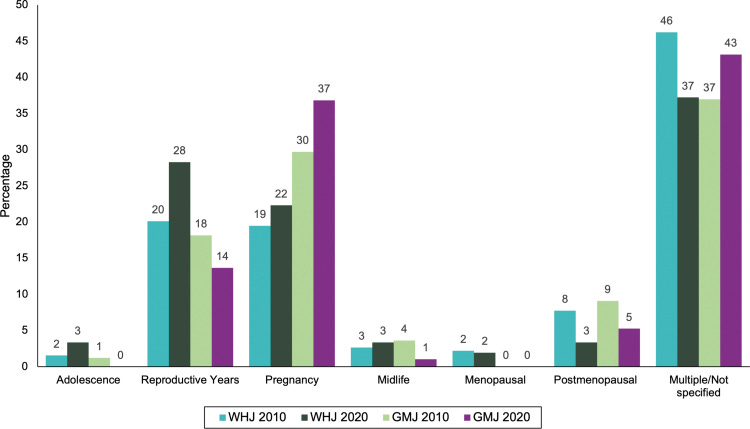
They also classified articles into the following life stages:
childhood (<10 years old),
adolescence (10–19 years),
reproductive years (15–50 years),
menopause (45–55 years)
midlife (45–60 years)
postmenopausal (>55 years)
When we base the research on life stage, we can see how minuscule attention midlife gets, including typical midlife (40-65) and menopause age (50-55). Post-menopausal includes older women, which has more research than the middle years. Although adolescence is also low, these journals are not the mainstay of adolescent research.
Goodbye to bikini medicine
People refer to mainstream medicine's focus on reproductive health as "bikini medicine." This implies that the only difference between men and women in terms of health is what is covered by a bikini. But this is simply isn’t true, as described in this paper:
This limited view of women's health, while covering important issues, excludes many of the main causes of mortality and morbidity for women, as well as the broad range of issues impacting women across the life span and around the globe.
Since I’ve started researching women’s midlife health, I’m focused on the number one killer of women: cardiovascular disease. But of course, heart disease looks different for women than men.
For instance, women are at higher risk for coronary microvascular dysfunction CMD, also referred to as "small vessel disease." This is a dysfunction of the small arteries, arterioles, venules, and capillaries.
Did you know that 50% of women that come into the emergency room with chest pain have minimal or no blockages? And many are reassured they are okay when they’re not?
That’s because they have non-obstructive coronary artery disease with no or little blockages in the large arteries. When people undergo further testing, it is discovered that 53% of those without blockages have CMD.
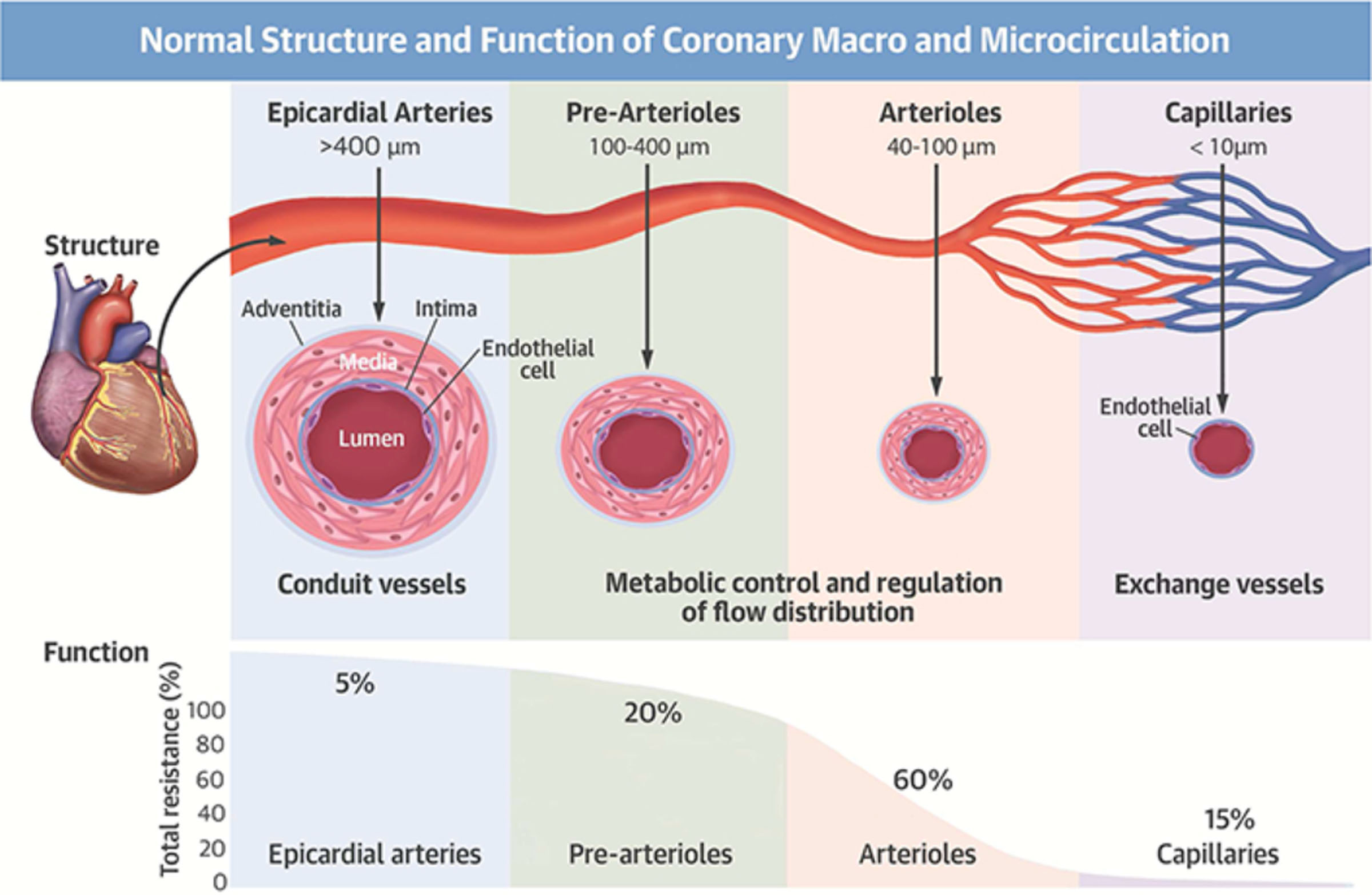
A majority (60%-75%) of people with coronary microvascular dysfunction are women – JAMA Network, 2019
So, yeah, let’s find out more about CMD and how it affects women and what we can do to decrease our risk (like now!)
Lung function is all but ignored
Also, the poor showing for respiratory diseases is shameful. At menopause, lung function decreases significantly and we’ve done so little to understand this.
For 20 years, researchers conducted a study with 1438 women aged 25-48. They measured hormone status and took information on menstrual patterns while testing lung function.
Forced vital capacity (measure of lung size) declined 10 ml/year in perimenopause and 12 ml/year in post-menopausal women. This was thought to occur due to increased inflammation in the lungs and osteoporosis, which can decrease breathing capacity by reducing the height of the chest vertebrae.
Menopause was found to be related to new-onset asthma and increased respiratory symptoms in a longitudinal population study.
“Whether obstructive or restrictive, the decline in lung function may cause an increase in shortness of breath, reduced work capacity and fatigue,” Said lead researcher, Kai Triebner in a press release. “Symptoms depend upon how much lung capacity is reduced, and a few women may actually develop respiratory failure as a result of this decline.”
This - and its connection to heart health - is why breathing exercise is one of the lifestyle factors in my book. I’m finding out all there is to help women improve their lung and breathing capacity. More on this in a future post.
Without adequate research, it’s the wild west
Without this foundation of research and formulation of guidelines, it’s easy for midlife-centered advice to get carried away. I’m on some private Facebook groups for midlife women and there are these accepted truths of which I cannot find research to support.
For instance, this idea that aerobic exercise is bad because it stimulates cortisol, increasing belly fat. What?
Given that our lung capacity and heart health are at risk, this isn’t a great idea.
What about the excessive promotion of protein to women? I’m not knocking protein, but some of these diet plans are missing vital micronutrients at the expense of protein, protein, protein.
And we can’t forget those who say hormone therapy will keep you from getting heart disease and dementia, which simply is not what the research says. WE need to move beyond estrogen as the answer for everything.
It seems like there’s so much noise while the core problems with our health are simply not being addressed. If you’ve heard some advice you’re not sure of, leave a comment or reply to this email (I might address it in a future post).
A call for more research
There is little doubt we NEED to step up midlife-related research. Chronic diseases common in older age are best addressed at midlife. And women are not little men.
I’ll leave with this call to action, the researchers state at the end of the paper. I sure hope someone is listening.
“We issue a call to action to research funders, publishers, and reviewers to broaden the focus of women's health and actively prioritize underresearched conditions as well as those comprising the greatest burden of disease in women globally, including NCD, communicable diseases, and injury.”